

5 min read
Diabetic neuropathies include a range of peripheral nerve dysfunctions that can be broadly categorized into generalized symmetric polyneuropathies and focal/multifocal neuropathies. Diabetic neuropathy (DN) is the most common long-term complication experienced by individuals with either type 1 diabetes (T1D) or type 2 diabetes (T2D). It stands as the leading cause of non-traumatic amputations and leads to significant morbidity, mortality, and economic burden. Approximately 30% of DN patients endure severe, debilitating pain that is largely unresponsive to current pharmacotherapies and persists for several years. DN pain is often localized to the feet, described as “burning” or “sharp,” and worsens at night or during periods of fatigue or stress. DN pain can be spontaneous and/or can be in the form of either allodynia (pain from a normally benign stimulus) or hyperalgesia (exaggerated pain from a normally mildly painful stimulus), or both. [1-3]
Hyperglycemia is a well-known contributor to DN pathogenesis, although advanced age, obesity, hyperlipidemia, and hypertension are also considered risk factors. While there is agreement within the biomedical research community that DN pathophysiology is multifactorial, there is no consensus yet as to the precise mechanisms of DN development and progression. Several potential pathophysiological mechanisms are currently under investigation, including activation of the polyol pathway, accumulation of advanced glycation end-products (AGE), oxidative stress, and neuroinflammation. To complicate matters further, these mechanistic pathways appear to be interrelated. [1-3]
Neuroinflammation
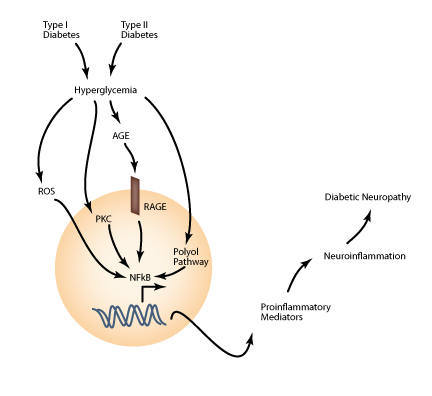
Highlighting neuroinflammation in the context of DN involves delving into a complex web of interacting cells and signaling molecules from both the nervous and immune systems. Neuroinflammation in the context of DN is initiated by various stimuli. Hyperglycemia directly activates protein kinase C (PKC), which has downstream effects, including the activation of the transcription factor NF-κB and the enzyme NADPH oxidase. NF-κB promotes the transcription of various pro-inflammatory genes, amplifying inflammatory signals in paracrine and autocrine fashions, recruiting circulating pro-inflammatory leukocytes, and promoting apoptotic cell death. NADPH oxidase further increases the production of reactive oxygen species (ROS), which are already elevated in the hyperglycemic environment. Regardless of their mode of production, ROS also directly enhance NF-κB transcriptional activity. Additionally, elevated AGE levels activate the AGE receptor (RAGE), which additionally promote NF-κB transcription of pro-inflammatory genes. Finally, metabolites in the polyol pathway can stimulate activation of PKC and thereby contribute to neuroinflammation as well. Figure 1 schematically illustrates how these interconnecting pathways converge to promote a pro-inflammatory transcription profile, initiating neuroinflammation—a major contributor to DN development and progression. [1,2]
Glycemic Control and STZ-Induced Models
The most effective means of preventing and treating diabetic neuropathy is glycemic control. There are currently only a few drugs approved for treatment of diabetic neuropathy and these drugs only function to relieve painful symptoms rather than curing the disease. Several drugs are currently in clinical trials, with many more in pre-clinical development. However, additional work is needed to further understand the mechanisms of disease onset and progression, and this research requires the use of experimental animal models. [1-3] Fortunately, there is already a wide variety of well-characterized rodent models of both T1D and T2D that develop complications including diabetic neuropathies that may be used to better understand the disease and develop more effective therapies.
While there is of course no single perfect animal model for human DN, the most commonly used model is the streptozotocin (STZ)-treated rat. [4,5] STZ is a cytotoxic agent derived from the gram-positive Streptomyces acromogenes bacterium that selectively kills pancreatic β-cells. Administering a single, low-dose STZ injection to healthy, adult rats results in their rapid development of a condition much like T1D in humans, where lack of functional β-cells in pancreatic islets impairs normal glycemic control. Treated animals become hyperglycemic within 72 hours of injection and develop significant neuropathic pain symptoms after approximately 4 weeks. Similar to other neuropathic pain models, the STZ rat model of diabetic neuropathy can be evaluated via a variety of quantitative behavioral tests for particularly mechanical allodynia and both mechanical and thermal hyperalgesia. [5]
The STZ rat model offers a number of important advantages over the other models of DN. Experimentally, the STZ rat protocol is relatively easy to execute, can be precisely controlled in terms of timing of the onset of diabetes symptoms, and consistently generates animals that are permanently and severely hyperglycemic. Further, there is a sizeable volume of published literature already available using this model, which offers researchers an important resource for comparing their findings to other laboratories and advancing their drug discovery efforts more quickly. Physiologically, the spontaneous nature of β-cell destruction in human T1D is very similar to what occurs in the STZ rat model and is thus likely more relevant for translational studies than some of the other models. For instance, the GK and ZDF rat models display no and only late hyperglycemia, respectively. Similarly, the ob/ob and db/db mouse models result from mutations in leptin and the leptin receptor, respectively, which are only very rare causes of T2D in humans. Pathologically, STZ rats exhibit serious hyperglycemia, are thus very ill, and suffer from severe DN symptoms. In terms of DN specifically, STZ rats exhibit reduced nerve conduction velocities, compromised endoneurial blood flow, aberrant calcium signaling and mitochondrial function, reduced nociceptive thresholds, activated apoptosis cascades, and indications of demylination and nerve degeneration. These pathophysiological changes result in quantifiable allodynia and hyperalgesia that serve as measures for testing new diabetic neuropathy treatment regimens. [4,5]
Patients with DN suffer from a range of pain symptoms that are chronic and progressive to the point of causing sleep disturbance, reduced mobility, incapacitation, and death. While meticulous glycemic control is the most effective method of preventing DN progression, it is the only method currently available for addressing the disease itself. All other approved pharmacological strategies merely serve to temporarily ameliorate symptoms and are only effective in a subset of patients. Further research is required to develop a more detailed understanding of DN pathophysiology so that new therapeutics can be developed to treat these patients. [1-3] Basic and pre-clinical research using experimental animal models is critical to this effort and the well-established STZ rat model has served and will continue to serve as an important translational model of human DN. [4,5]
Interested in working with our research group? Contact us here.
References
- Tahrani, A.A., Askwith, T., and Stevens, M.J. (2010). Emerging drugs for diabetic neuropathy. Expert Opinion on Emerging Drugs, 15(4):661-683.
- Mahmood, D., Singh, B.K., and Akhtar, M. (2009). Diabetic neuropathy: therapies on the horizon. Journal of Pharmacy and Pharmacology, 61(9):1137-1145.
- Ziegler, D. (2009). Painful diabetic neuropathy: advantage of novel drugs over old drugs? Diabetes Care, 32(Suppl 2):S414-S419.
- Sigaudo-Roussel, D., Fromy, B., and Saumet, J.L. (2007). Diabetic neuropathy in animal models. Drug Discovery Today: Disease Models, 4(1):39-44.
- Morrow, T.J. (2004). Animal models of painful diabetic neuropathy: the STZ rat model. Current Protocols in Neuroscience, 9.18.1-9.18.11.
Related Posts
A minipig Model of Incisional pain
The use of animal models for the research of post-operative pain (POP) has been well described[1]....